Severe peripheral artery disease can present with rest pain or ulcerations or even gangrene. This is known as critical limb ischemia. Critical limb ischemia is most often not a medical emergency, but sometimes complications of critical limb ischemia lead to the need for leg amputation. A decision regarding the need for amputation and the level of amputation is not always straightforward. The following are some of the considerations when deciding about the need for amputation and about the level of amputation in patients with critical limb ischemia:

3rd toe gangrene and two areas of yet undemarcated ischemia on the dorsum of a left foot
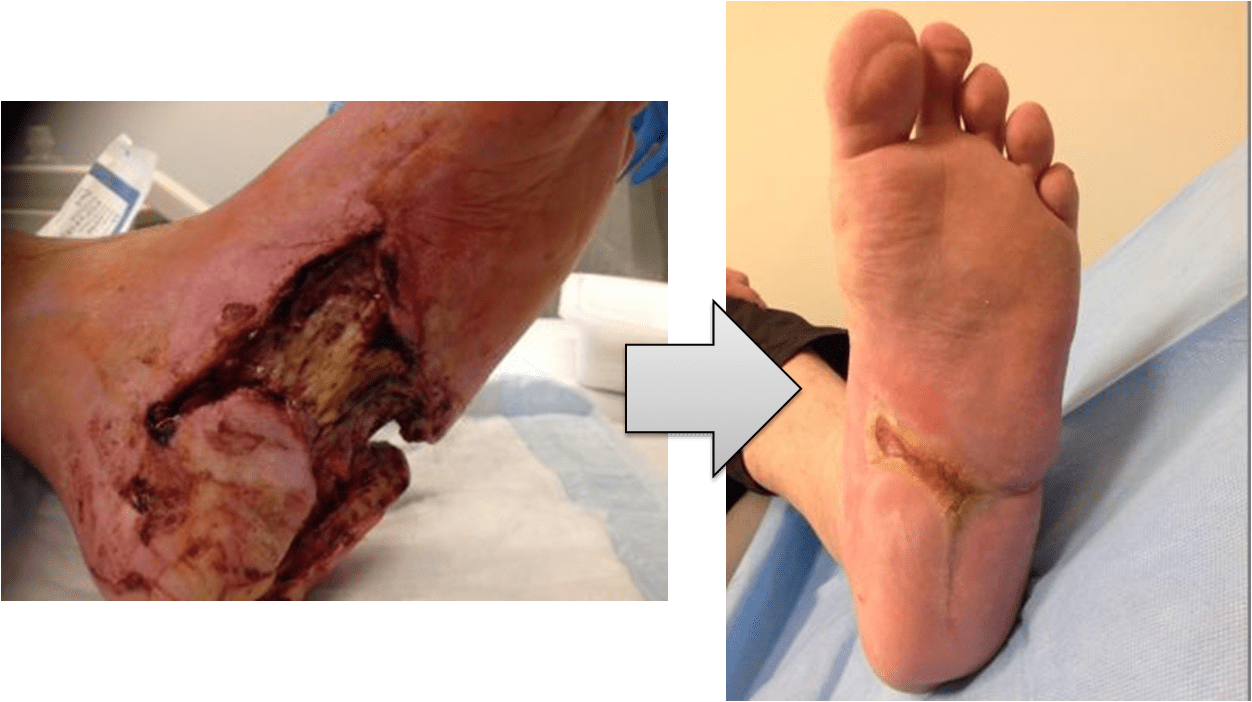
With excellent wound care, even this wound healed
-
Severity of ischemia – Perhaps the most important factor when trying to predict whether a wound will heal or not is the degree of blood flow to the wound bed. Patients with multilevel arterial disease who have severely reduced ankle or foot pressures have very little chance to heal a wound. Furthermore, lack of blood flow to a specific area of the foot, may impede wound healing in that particular area. This is called the ‘angiosome theory‘. While some believe that cross-collateralization may be sufficient to heal wounds, others think that direct, inline, flow to the wound bed is needed for appropriate healing.
It is important to note that no one system is perfect in assessing perfusion to a wound bed. Measures that are in clinical use include the ankle pressures, toe pressures and TcPO2. Many companies have attempted to produce a device that would analyze microcirculation in an intuitive, non-invasive manner.
- Degree of tissue loss – Degree of tissue loss is measured by a combination of depth and area of the wound. Larger and deeper wounds have a lower healing rate compared to smaller, more shallow wounds. Furthermore, a wound that has progressed to gangrene has less chance of healing than a wound that still harbors viable tissue. Tissue loss is among the variables that is most strongly associated with risk for amputation. It is noteworthy that recognition of the extent of gangrene is not alway easy. Sometimes dark discoloration of tissue may still be reversible, while at other times gangrene demarcates progressively with time.
- Superimposed infection – Infection is perhaps the most common reason for emergent amputations. Patients who suffer from severe peripheral artery disease have a reduced capability to fend off infection, as there is less blood supply to the affected area. Thus, even the most mundane infection (e.g. ingrown toenail) can progress rapidly to florid cellulitis and deep skin infection. Also, antibiotics, that often rely on proper blood flow for tissue penetration as well as on local pH for activation, may be less effective as ischemia worsens. Thus, gangrene with superimposed deep tissue infection (e.g. osteomyelitis), especially when revascularization is not possible, often results in amputation. Obviously, the depth and extent of infection should play a role in making the decision, with deeper, more widespread infections suggesting a greater chance of amputation. There are several scoring systems that combine the degree of ischemia, wound area and depth and the presence of infection into a scoring system that predicts the chances of amputation. Recently, a system called WIfI has been proposed by the society for vascular surgery.
- Available wound care expertise – Appropriate wound care is central for avoiding amputation, specifically in those instances when it can be avoided. Patient and family cooperation are usually paramount. Next, the ability to offload the affected foot to reduce pressure injury. This is done by a combination of expert footwear (usually provided by podiatrists with specific expertise in the field) and by the use of crutches and a wheelchair for mobility. Then, there is specific intensive wound care. This is usually best provided by expert wound care centers that can identify progress or complications and react accordingly by changing their therapeutic strategy or by referring patients for acute care if superinfection is suspected.
- Chances for rehabilitation – It may come as a surprise to some readers, but amputation is sometimes the better rehabilitation alternative for patients as compared with prolonged wound care and repeat local procedures. Also, compared to bypass, amputation is a lower risk surgery (when an endovascular approach is impossible). As patients who need amputation are often systemically frail(i.e. coronary artery disease, chronic kidney disease etc.), choosing the less aggressive of options may lead to more favorable outcomes. Furthermore, with modern rehabilitation techniques, and motivated patients, post-amputation rehabilitation may produce a high quality of life and close to normal independence.