
- Osteomyelitis
-
by tmi
DPM, MPH
PRESENT Editor,
Diabetic Limb Salvage
Osteomyelitis- Making the Diagnosis
I n this month’s issue, we will discuss an ostensibly difficult topic that we all face when managing patients with diabetic foot ulcers – that of underlying osteomyelitis(OM). Perhaps no other related topic is faced with as much consternation as is this. Osteomyelitis (bone infection) specifically refers to infection of the medullary bone as opposed to osteitis wherein the periosteum or cortical surface becomes infected through a penetrating wound or ulcer. Despite these differences, the two are clinically diagnosed or treated in much the same way. Having treated osteomyelitis (OM) associated with diabetic foot wounds for many years, I certainly recognize what a conundrum it can be for the clinician. Since both diagnosis as well as treatment can be clinically challenging, let’s just focus on its diagnosis this month. We’ll get to management next month.
Much has been written about the diagnosis of OM over the years and especially that which complicates diabetic foot ulcers (DFU).1-3 Whereas hematogenous osteomyelitis generally affects children, OM complicating the diabetic foot almost always arises from a contiguous penetrating wound or foot ulcer. There are several ways to classify OM, but the most popular way in academic circles is the Cierny-Mader classification that attributes both an anatomical (diffuse, localized, etc.) as well as host status (healthy, compromised, etc.) components.4 Although this can be helpful in categorizing the bone infection, in the feet of patients with diabetes, osteomyelitis is usually chronic and difficult to effectively treat. Hence, early diagnosis becomes a critical factor in its successful management.
As in most disorders, clinical suspicion for this complication is paramount in making the diagnosis early. If one suspects OM or routinely makes an effort to investigate its presence (or absence), one is more likely to detect it when indeed present. Generally speaking, ulcers of greater duration, depth, or size have a higher likelihood of developing underlying OM. This has been confirmed in some studies and not corroborated in others, so these wound characteristics are not definitive markers. Nonetheless, it is always wise to suspect bone infection under indolent ulcers and particularly so in patients with peripheral arterial disease(PAD). A very important concept to introduce into our discussion at this point is that of prevalence or prior probability of the disease. Much has been made of prior probabilities in recent years, especially in the interpretation of diagnostic tests.5,6 For example, in the routine outpatient setting, one can expect to see relatively uncomplicated (healthy appearing) neuropathic DFUs. While I hesitate to use the term “healthy”, a neuropathic ulcer of fairly recent onset (let’s say 4 weeks in duration) that is superficial, granular, and well perfused without evidence of infection has a relatively low prevalence of osteomyelitis (perhaps 20% or so).6 Bayes theorem suggests that any diagnostic test will have a higher rate of false positive results when the prevalence of disease is low. Contrast the outpatient scenario above with that of
the inpatient setting wherein patients with acutely infected foot ulcers are admitted. These patients might also have associated PAD as well and by the nature of their active infection, their prevalence of associated osteomyelitis might be in the range of 66 to 95%, depending upon the study one relies upon.7,8,9Therefore, positive findings on clinical, laboratory, and imaging examinations are more likely “true” positives than false positive findings (unless there is an associated Charcot foot). Accordingly, when interpreting published studies, as always, we must be mindful of the patient population under study. This seemingly obvious fact has lead to most of the published controversy in ascertaining the accuracy of various diagnostic tests in this regard.
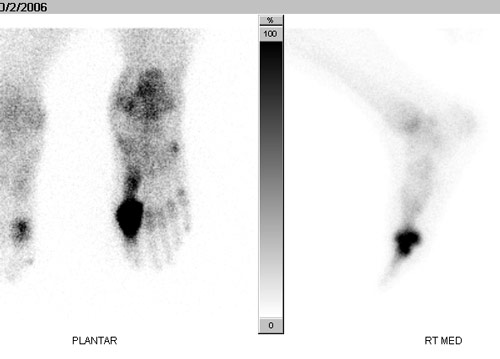
We are all well familiar with the role of various imaging modalities in the diagnosis of osteomyelitis and certainly, much has been written on them in the setting of the diabetic foot.10-12 While I will refer the reader to the list of references for detailed reviews of diagnostic imaging, let me briefly summarize the pros and cons of the more common modalities used in detecting OM complicating diabetic foot ulcers. First and foremost, we must always take Xrays . Plain radiography is readily available around the world, inexpensive and can provide essential information at the onset of patient contact. We look for foreign bodies, soft tissue swelling, gas, fractures, and erosions or periosteal new bone formation- the latter two being suggestive for osteomyelitis in the infected foot. Unfortunately, Xrays are very insensitive to OM because the visible changes are often delayed or the two dimensional image might not ascertain a focus of osteomyelitis under a central metatarsal head or calcaneus until very late in the course of the disease. However, when radiographic changes are evident directly under an ulcer with visible bone at its base, the diagnosis becomes highly likely. Three phase technetium (99mTc) bone scans, on the other hand, are highly sensitive scintigraphic scans, but suffer due to poor specificity, especially in the setting of neuropathy. Hyperemia of bone due to autonomic neuropathy, neuropathic bone changes, and minor stress fractures can result in false positive findings. Therefore, these bone scans are usually combined with leukocyte scans (i.e. indium scans) that are more specific (although not 100% accurate) for bone infection.

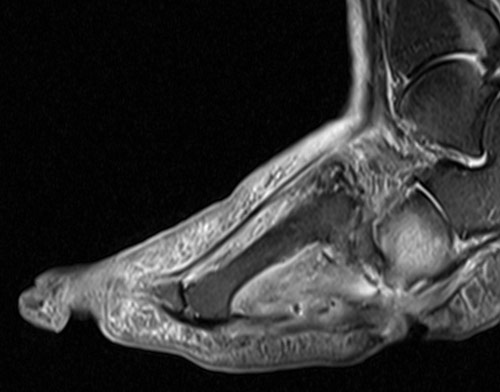
MRI is presently considered to be the most accurate imaging modality to ascertain underlying osteomyelitis, especially when using special sequences (fat suppression) or contrast media (gadolinium). Nonetheless, in the presence of underlying neuropathic bone changes (Charcot arthropathy), the diagnosis of osteomyelitis becomes more difficult is certainly less accurate.11 Computed tomography ( CT), SPECT, and PET/CT are also interesting modalities in this regard, but the latter are not yet widely available and there is not a lot of published data on their utility in the diabetic foot.10
For years, my most useful clinical examination technique has been the Probe-to-Bone (PTB) test.

Figure 4. The Probe to Bone test using a simple applicator stick. This is positive when bone or a hard, gritty surface is palpated.
First brought to the forefront by Grayson in 1995, this simple clinical evaluation technique yielded an 89% positive predictive value (PPV) in patients hospitalized with diabetic foot infections and a prevalence of osteomyelitis of 66%.5 As inferred earlier, the utility of this test has come under scrutiny, especially in the outpatient setting, because of the high prevalence of osteomyelitis in this hospitalized population. Another study that reported on the PTB test in a primarily outpatient population found a much lower PPV of 57% in patients with foot ulcers (clinically infected and uninfected).6 The prevalence of osteomyelitis in their cohort of infected foot ulcers was 20%. Unfortunately, confirmation of osteomyelitis was obtained only by bone culture and not histopathology. Despite the questions raised by this study, I continue to probe each and every wound, especially deep wounds, to ascertain whether a hard or gritty bone surface can be palpated with a sterile, blunt instrument (even the back of an applicator stick). I call this (as suggested by a colleague years ago) my “five cent bone scan”. When bone is palpated, I consider the patient to have clinical osteomyelitis or osteitis and will investigate further with cultures and imaging for confirmation. Although false positives can occur, I consider them to be fairly infrequent.
Several recent studies have confirmed the utility of the PTB test in diagnosing biopsy proven osteomyelitis, indicating a positive predictive value of 95 to 97% (often combined with plain radiography) in patients with clinically infected foot ulcers.8,9 Interestingly, the same authors who refuted the value of the PTB test in the outpatient ulcer population (above), in a subsequent study reported that the strongest independent risk for osteomyelitis was imparted by wounds that extended to (probed to) bone with a relative risk of 23.1.13 Therefore, it seems to me that the probe to bone test is a simple, efficient, and reliable test that can be done at bedside to indicate the likelihood of osteomyelitis underlying diabetic foot ulcers. In concert with appropriate imaging, the diagnosis can therefore be made sooner and facilitate earlier treatment – stay tuned for next month’s discussion on management of osteomyelitis!As always, we encourage discussion and hope that you will feel free to let us know what you think. I also welcome your suggestions for future FootNotes.
References are provided below that can expand upon many of the points made above. We welcome your opinions, concerns, and suggestions. If you have an interesting case or a troubling circumstance that you would like to share with fellow PRESENT Diabetes members, please feel free to comment on eTalk.
Best regards,
Robert Frykberg, DPM, MPH
PRESENT Editor,
Diabetic Limb Salvage
REFERENCES![]()
- Frykberg RG: An evidence-based approach to diabetic foot infections. American Journal of Surgery. 186 (Suppl 1):44-54, 2003
- Frykberg RG, Wittmayer B, Zgonis T: Surgical Management of Diabetic Foot Infections and Osteomyelitis. Clinics Podiatr Med Surg. 24: 469-482, 2007
- Thomas-Ramoutar C, Tierney E, Frykberg R : Osteomyelitis and Lower Extremity Amputations in the Diabetic Population. The Journal of Diabetic Foot Complications: 2010, 2 (1), No. 4, pp. 18-27.
- Cierny III G, Mader JT,Penninck JJ: A clinical staging system for adult Osteomyelitis. Contemp Orthop 10:17–37, 1985
- Wrobel JS, Connolly JE. Making the diagnosis of osteomyelitis. The role of prevalence.J Am Podiatr Med Assoc88(7):337-43, 1998
- Lavery LA, Armstrong DG et al: Probe-to-Bone Test for Diagnosing Diabetic Foot Osteomyelitis. Diabetes Care 30:270–274, 2007
- Grayson et al: Probing to bone in infected pedal ulcers. JAMA March 1995 273: 721-723
- Lozano et al: Validating the Probe-to-Bone Test and Other Tests for Diagnosing Chronic Osteomyelitis in the Diabetic Foot. Diabetes Care 33:2140–2145, 2010
- Aragon-Sanchez J et al: Diagnosing diabetic foot osteomyelitis: is thecombination of probe-to-bone test and plain radiography sufficient for high-risk inpatients? Diabet. Med. 28, 191–194 (2011)
- Termaat MF, Raijmakers PG, Scholten HJ, Bakker FC, Patka P, Haarman HJ. The accuracy of diagnostic imaging for the assessment of chronic osteomyelitis: a systematic review and meta-analysis. J Bone Joint Surg Am87(11):2464-71, 2005.
- Sella EJ, Grosser DM. Imaging modalities of the diabetic foot. Clin Podiatr Med Surg20(4):729-40, 2003
- Lew DP, Waldvogel FA. Osteomyelitis. Lancet364(9431):369-79, 2004.
- Lavery L, Peters E et al: Risk factors for developing osteomyelitis in patients with diabetic foot wounds. Diabetes Research Clinical Practice 8 3 ( 2 0 0 9 ) 3 4 7– 3 5 2