- Charcot
-
by tmi
Charcot Neuroarthropathy
Case Study, Part 1
Jeffrey Siegel, DPM, FACFAS, DABPO
Adjunct Assistant Professor, Depts. Of Medicine and Surgery, TUSPM
 |
A 78 year old WF presents to the office for a second opinion regarding her severely deformed right foot. Mrs. B states that 6 months ago she was diagnosed with a diabetic ulcer on the medial arch that required two procedures to close. Patient denied ulcerations on the bottom of her foot. Over this time period, her foot had become progressively deformed, swollen, red and painful when she walks. Mrs. B stated that “I was told that I have Charcot foot and that I have to live with it because nothing can be done.” Past treatment included: Non-weight bearing and custom molded shoes. Her BS ranges from 80 – 160. States that she was diagnosed with diabetes just two years ago, but has had numb feet for years. Mrs. B. uses a cane normally and her post-operative goal is to be able to perform her normal activities of daily living.
Allergies: NKDA.
Medication History: Actos, Aspirin, Caltrate 600 with D, Carvedilol, Centrum Silver, Ferrous gluconate, Fish Oil, Levothyroxine, Lisinopril, Magnesium carbonate, Neurontin, Warfarin.
Past Medical History: Cardiovascular Hx: (+) hypertension (HBP), (+) pacemaker.
Musculoskeletal Hx: (+) arthritis conditions.
Hematologic / Lymphatic Hx: (+) anemia.
Endocrine Hx: NIDDM x 2 yrs.
Past Surgical History: Insertion of dual chamber pacemaker; right 2nd toe amputation and debridement right arch (medial cuneiform) and a second debridement for wound dehiscence.
Social History: Patient denies smoking, alcohol abuse, illicit drug use, and STDs.
Family History: Unremarkable.
Review of Systems: Unremarkable with exception of chief complaint and all other systems are negative.
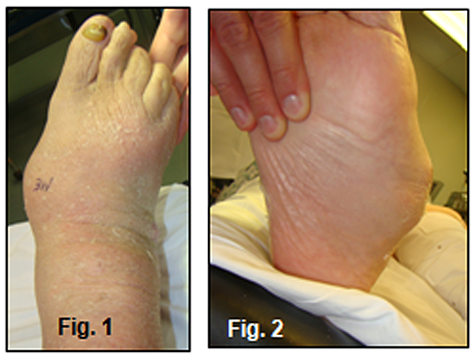
Physical Exam: Examination revealed evidence of a Lisfranc’s deformity with complete collapse of the foot yielding a very prominent medial midfoot and rigid, laterally deviated forefoot (Figure 1,2).
 |
There is a well healed incision over the medial cuneiform (Figure 3).
 |
The foot has mild edema and erythema and there is no lymphangitis, adenopathy or open lesions. There is, however, an area of fluctuance over the dorsolateral midfoot that when aspirated, yielded 5 cc’s of an opaque, blood tinged fluid (Sent for C & S).
Vascular: DP/PT pulses are 2/4, bilateral. Capillary fill time is immediate. No contralateral lower-extremity edema is noted and varicosities were not observed.
Derm: Skin temperature of lower extremities warm to warm proximal to distal. Skin inspection was otherwise unremarkable. Mycotic changes noted in the nails 1-5 bilateral.
Neuro: The 5.07 monofilament test was performed and there was profound evidence of loss of protective sensation. Touch, pin, vibratory, and proprioception sensations were abnormal. Deep tendon reflexes diminished.
Ortho: Examination of the patient’s ankle joint dorsiflexion reveals limitation of dorsiflexion of foot relative to leg with knee extended AND flexed consistent with gastroc-soleal equinus deformity. There is loss of stability of the foot with significant hypermobility and excessive dorsiflexion and abduction of the midfoot. Crepitus noted with ROM consistent with an acute vs. chronic Charcot deformity. Muscle strength 5/5 for all groups tested. Muscle tone normal. Mild genu valgus B/L. Inspection and palpation of bones, joints, and muscles otherwise unremarkable.
Diagnostic Studies: Non-weight bearing plain films and 3D CAT Scans: Evidence of a displaced, comminuted fracture-dislocation of the Lisfranc joint w/collapse of the medial cuneiform and severe lateral deviation of the forefoot (Figure 4-6). Hypertrophic degenerative changes are present in the midfoot. The pre-op lateral view is partial weight bearing which explains the normal appearing talocalcaneal relationship vs. post-op weight bearing views. There is some rounding and sclerosis at the 1st TMT joint. Osteolytic changes are seen in the body of the cuboid consistent with acute Osteomyelitis (Fig. 4). CAT Scan evidence plantar and medial displacement of the medial cuneiform and collapse of the cuboid (Figure 7-8). Hindfoot and ankle views are WNL.
 |
 |
|
###
|